

Ngā Kōrero a te Poari: Maxine Ketu
Our Board Member Maxine Ketu (Ngāti Maniapoto, Waikato-Tainui), shares whakaaro on improving health outcomes for whānau and communities.
Why this kaupapa?
Firstly, why me?
I was appointed Pouārahi/General Manager of Ngāti Hāua Iwi Trust with a key focus on supporting our Trustees through the completion of our Treaty Settlement journey.
As that role evolved, I was appointed to the Waikato DHB Iwi Māori Council, and over the years I have continued alongside the evolution of Māori health representation to where we are today with Te Tiratū.
The responsibility I carry when representing Ngāti Hāua and our rohe is significant. For me, this mahi is about the difference between life and death for our people.
That understanding comes from lived experience. My own whānau experienced the impacts of rural isolation, poverty, limited access to healthcare, and the inequities Māori continue to face within the health system. Those realities contributed to the untimely loss of a loved one.
That was 11 years ago, but since 2014 I have walked beside many whānau who have experienced the same pain and loss. I have woven waka wairua for whanaunga taken too young, too soon. I have stood at nehu and helped lay our loved ones to rest when I know they should still be here.
My representation, my passion, and my commitment to this kaupapa all come from those lived experiences.
What does real change look like?
Real change starts with whānau feeling empowered to take charge of their own health and wellbeing. That looks like:
- having access to good health education and information
- understanding our own whānau and generational health histories
- feeling confident to ask questions and seek second opinions when needed
- not settling for poor treatment or mediocre care
- putting ourselves and our loved ones first
- making informed and healthy choices through ongoing learning
- knowing we have the right to demand high-quality care for ourselves and our whānau at all times
Real change also means the health system valuing the mātauranga, lived experiences and voices of whānau as part of healthcare assessment, treatment and follow-up.
We need a health workforce that is trained to recognise and address unconscious bias. This learning should not be optional, it should be embedded across all health education, professional training and ongoing development.
For our rural communities, real change means equitable access to healthcare no matter where you live. Communities that are far from hospitals and specialist services need secure, long-term investment that is protected across governments and political cycles. Rural whānau should not receive poorer outcomes simply because of where they live.
We also need stronger systems for accountability and learning. A national complaints and feedback system could help ensure concerns raised by whānau are heard, responded to, and used to improve services over time. The information gathered could help identify gaps in access, improve service delivery, strengthen professional practice, and ultimately lead to better health outcomes for our people.
What needs to stop, shift or grow?
We need to stop accepting inequitable outcomes for Māori and rural communities as normal.
The health system must be shifted toward one that truly listens to whānau, values Māori knowledge, and responds with compassion, accountability and equity.
We need to grow:
- investment in iwi-led health education and prevention
- culturally safe healthcare practices across the system
- unconscious bias training throughout health education and workforce development
- diversity within the health workforce, so our people can see themselves reflected in the system
- better access to healthcare services for rural communities
- stronger systems for listening and responding to whānau feedback and complaints
When whānau feel seen, heard, respected and supported, health outcomes improve. That is the future we should all be working toward.
Pharmac proposes removing priority access of type 2 diabetes meds for Māori, Pasifika
Associate Professor Dr Ryan Paul, a clinician and technical expert advisor to Te Tiratū, has expressed serious concern in an interview with 1News about proposed changes to funding criteria for type 2 diabetes medicines. He warns that removing ethnicity-based access pathways could deepen existing inequities for Māori and Pacific peoples.
The proposed Pharmac changes would expand general access to medicines such as empagliflozin, liraglutide, and dulaglutide, but would remove targeted pathways that currently acknowledge the higher burden of diabetes, cardiovascular disease, and kidney disease experienced by Māori and Pacific populations.
Te Tiratū co-chair Glen Tupuhi notes that equity-focused pathways were introduced because the health system has repeatedly failed to deliver fair outcomes for Māori, who are diagnosed earlier, experience more severe disease, and have higher rates of premature mortality from preventable long-term conditions.
Māori clinicians and health leaders have cautioned that the proposed shift could undo one of the most effective equity interventions introduced in recent years.
The consultation closes on 28 May 2026.

Māori health leaders warn proposed Pharmac changes could deepen inequities and cost lives
Te Tiratū has spoken with Whakaata Māori with serious concerns about proposed changes to access criteria for funded type 2 diabetes medicines, warning the removal of ethnicity-based pathways could worsen long-standing inequities for Māori and Pacific peoples.
The proposed changes by Pharmac would widen general access to medicines including empagliflozin, liraglutide and dulaglutide, but remove the current pathway that recognises the disproportionate burden of diabetes, cardiovascular disease and kidney disease experienced by Māori and Pacific communities.
Te Tiratū co-chair Glen Tupuhi says equity pathways exist because the health system has consistently failed to deliver equitable outcomes for Māori, who are diagnosed younger, experience more severe illness, and die sooner from preventable chronic conditions.
Associate Professor Dr Ryan Paul, clinician and expert technical advisor to Te Tiratū, said he was “really gutted” by the proposal, particularly given the success of the current pathway in improving equitable access to life-saving medicines for Māori and Pacific whānau.
Māori clinicians and health leaders warn the proposal risks reversing one of the most successful equity interventions introduced in recent years.
The consultation closes on 28 May 2026.

Pharmac proposes removing priority access of type 2 diabetes meds
Te Tiratū Iwi Māori Partnership Board co-chair Glen Tupuhi and expert advisor, researcher Dr Leanne Te Karu have spoken to RNZ about growing concerns over Pharmac’s proposal to remove ethnicity-based access criteria for type 2 diabetes medicines, despite new evidence showing significant life-saving benefits for Māori and Pacific communities.
In the interview, Dr Te Karu said the original criteria were introduced because Māori and Pacific peoples were not receiving equitable access to treatment through the health system, despite experiencing higher rates of diabetes, earlier onset disease, and more severe complications.
She said the medicines had been shown to improve equity outcomes and narrow survival gaps, warning that removing the criteria before systemic inequities are addressed risks widening disparities again.
Te Tiratū co-chair Glen Tupuhi said that treating everyone the same within an inequitable system does not create fairness, but instead entrenches inequity. Te Tiratū is filing a submission to Pharmac calling on it to reconsider the proposal and ensure equity remains central to decision-making for whānau experiencing the highest health burden.

Māori mental health inequities in Waikato demand urgent system reform
Te Tiratū represents approximately 121,000 Māori across the Waikato rohe, with around half under the age of 25. In our submission to the Government’s Mental Health and Wellbeing Strategy filed today we said the national mental health policy must be built from the realities of rangatahi Māori and whānau Māori and not retrofitted to them.
In rural Waikato, distress is not abstract. It is shaped by access barriers, workforce shortages, housing and income pressure, and the compounding effects of isolation. Te Tiratū argues that unless these conditions are addressed directly, the mental health system will continue to respond too late, and too often in crisis.
Our core message to Government
Te Tiratū is calling for a strategy that shifts from crisis response to prevention, from generic service design to Māori-led solutions, and from urban-centric planning to rural equity.
Our submission’s most critical recommendations are:
- Increase rural funding and expand telehealth capacity.
- Build and retain a rural mental health workforce.
- Address socioeconomic drivers of distress.
- Resource Māori cultural perspectives and whānau involvement.
- Support youth-led and community-based programmes.
The evidence from Tainui Waka Rohe
Our submission draws on our locality evidence base, which shows persistent and significant inequities in mental health outcomes across our region.
- Between 2017 and 2022, 16.0% of Māori aged 15+ in Waikato District experienced high or very high psychological distress
- Rising to 19.7% for Māori women
- Māori were 1.7 times more likely than non-Māori to experience high or very high distress
The data also shows the depth of unmet need:
- 5% of Māori reported a depression diagnosis
- 1% reported an anxiety disorder
- Māori were 1.9 times more likely than non-Māori to be hospitalised for mental or substance use disorders (2020–2023)
- Including 4.6 times higher hospitalisation rates for schizophrenia
- Around 225 Māori aged 15 to 44 are hospitalised each year for intentional self-harm
What must change in the system
We believe the current system is still too weighted toward crisis care, with insufficient investment in early intervention, rural access, and culturally grounded support.
Our submission says that meaningful improvement will only occur when services are designed closer to communities, delivered earlier, and shaped by a te ao Māori worldview and leadership.
We know workforce retention in rural areas is a critical pressure point because without it, access gaps will persist regardless of funding increases.
Treaty obligations and system accountability
A key concern of our submission is the limited visibility of Te Tiriti o Waitangi within the draft strategy, particularly Article 3 obligations relating to equity.
Without explicit Te Tiriti grounding, the strategy risks failing to address the structural drivers of inequity in mental health outcomes for Māori.
How accountability, investment, and service design are structured determines whether equity is achieved or not.
National context reinforces urgency
National data from Te Hiringa Mahara – Mental Health and Wellbeing Commission confirms the same pattern seen in Waikato, with 22.5% of Māori adults experiencing high or very high psychological distress, and 22.9% of young people aged 15–24 affected.
This aligns strongly with our locality findings and reinforces that rangatahi Māori are carrying a disproportionate burden of distress across the country.
Strategy alignment, but not yet sufficient
Our submission responds to the Ministry of Health New Zealand Draft Mental Health and Wellbeing Strategy 2026–2036, which focuses on prevention, access, workforce, and quality of care.
We support these directions in principle but argues they will not succeed unless they are explicitly grounded in Te Tiriti, rural equity, and Māori-led service design. Without this, the strategy risks maintaining existing inequities under a restructured framework.
Mental health reform will not succeed in Tainui Waka rohe if it continues to treat Māori as an “equity consideration” rather than the foundation of system design. The evidence shows that inequities are persistent, and the solutions are known. What is required now is investment, accountability, and a shift in power toward Māori-led, whānau-centred, community-based approaches.
Important References to inform the strategy:
- Te Tiratū IMPB, Hauora Māori Priorities Summary Report, here, pp.36-41 – Waikato Māori psychological distress, depression, anxiety, suicide, mental health hospitalisations, substance/alcohol-related hospitalisations and intentional self-harm data.
- Te Tiratū IMPB, Monitoring Report to March 2025 here, 15 May 2025, pp.22 and 25-26 – Māori access to primary and specialist mental health and addiction services, ED mental health waits, and commentary that services must remain culturally safe and whānau-friendly.
- Te Tiratū IMPB, Position Statement – Rangatahi Māori Mental Health, here23 September 2025 – Te Tiratū public position on rangatahi Māori mental health in rural Waikato, including rising distress, suicide risk, addictions, takatāpui youth pressures, rural isolation, service gaps, and the call for kaupapa Māori, whānau-led solutions.
- Te Hiringa Mahara – Mental Health and Wellbeing Commission, NZ Health Survey 2024/25 mental health and substance use data summary, 25 February 2026 – national context: 22.5% of Māori adults and 22.9% of young adults aged 15-24 experienced high or very high psychological distress.
- Ministry of Health, Draft Mental Health and Wellbeing Strategy 2026-2036 consultation, 8 April 2026 – consultation context and the four priority areas: prevention and early intervention, improved access, supported workforce, and quality/effectiveness of care.

Equity at risk? Call to retain ethnicity criteria for key diabetes medicines
In a recent opinion piece in Pharmacy Today and NZDoctor by our expert advisor on prescription medicine Dr Leanne Te Karu warns that proposed changes by Pharmac could make health inequities worse for Māori and Pacific whānau.
Pharmac is thinking about removing a rule that helps Māori and Pacific peoples get better access to important diabetes medicines like SGLT2 inhibitors and GLP-1 receptor agonists.
Right now, Māori and Pacific peoples are more likely to get diabetes earlier, get sicker faster, and not always get the same access to the medicines and care they need. The current system was designed to help fix this by making sure people who need it most can get these medicines sooner.
Evidence shows this approach has been working, more Māori and Pacific peoples have been able to access treatment, and it has helped improve health outcomes and survival.
Removing this support before the wider system is fixed could mean going backwards.
Submissions close 28 May. This is a chance to speak up for fair access to life-saving medicines for our whānau.

Pharmac proposal to remove ethnicity criteria criticised
Pharmac is facing strong criticism in NZDoctor and Pharmacy Today over a proposal to remove ethnicity as a criterion for access to several diabetes medicines, with opponents warning the change could lead to more Māori and Pacific deaths and deepen long-standing inequities in the health system.
The proposal would amend Special Authority settings that currently prioritise access for groups disproportionately affected by type 2 diabetes, including Māori and Pacific peoples who experience higher rates of earlier onset and more severe complications.
Te Tiratū Iwi Māori Partnership Board was quoted by both publications because we say removing ethnicity equity criteria raises serious concerns about whether Pharmac is meeting its obligations under Te Tiriti o Waitangi to achieve equitable Māori health outcomes.
We are warning that “treating all universally in the system does not create fairness. It entrenches inequity.”
Our board is calling for Pharmac to retain ethnicity-based access criteria, publish its equity impact analysis before consultation proceeds, clearly demonstrate how Māori health outcomes would improve under the proposed change, and engage directly with iwi Māori partnership boards, Māori clinicians and Māori health providers.
Submissions on the consultation close on 28 May 2026 leaving just 13 days for feedback on a proposal that critics say could reshape access to essential diabetes treatment.
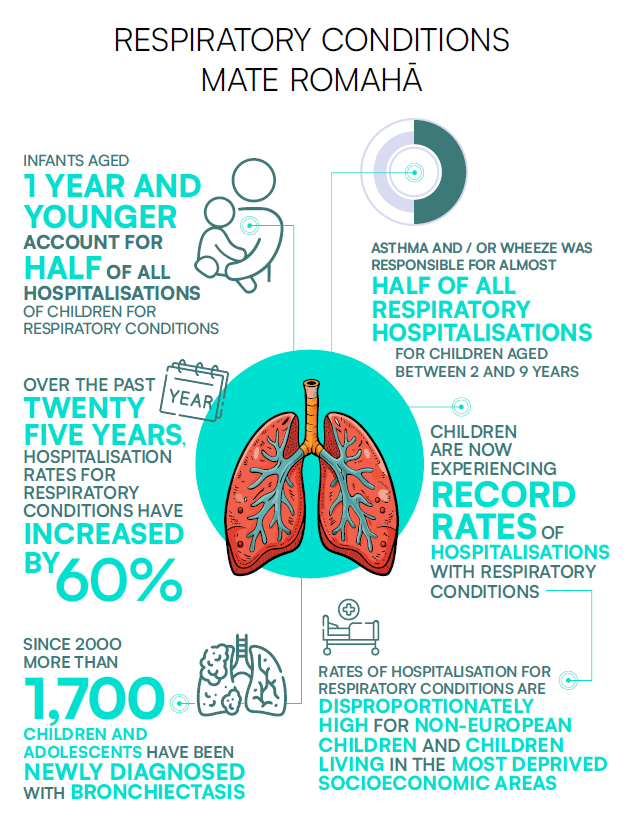
60,000 children hospitalised each year with preventable illness
Te Tiratū Iwi Māori Partnership Board is backing urgent calls for action following the release of the fifth State of Child Health in Aotearoa New Zealand Report, which highlights worsening child health outcomes and persistent inequities for tamariki Māori.
The report, produced by Cure Kids in partnership with the New Zealand Child and Youth Epidemiology Service at the University of Otago, shows around 60,000 children are admitted to hospital every year with illnesses considered preventable.
Respiratory hospitalisations have increased by 60 percent since 2000, with babies under one year old accounting for almost half of all admissions. Tamariki Māori continue to experience disproportionately high rates of respiratory illness and rheumatic fever.[1]
These national trends are already being felt across Tainui waka rohe. Local monitoring shows an average of 215 Māori children aged 14 and under were hospitalised for asthma each year in Waikato District between 2020 and 2023 1.9 times the rate of non-Māori children.
The figures reflect the wider realities many whānau are living with. Nearly half of Māori in Waikato DHB lived in the two most deprived deciles, almost one in four lived in overcrowded housing, 45 percent reported damp homes, 37.2 percent reported mould, and an estimated 17.5 percent of Māori were not enrolled with primary care.[2]
For rural whānau, the pressures are often even greater. Long travel distances, transport barriers, workforce shortages and delayed access to care can quickly turn manageable illness into hospital-level illness.
Te Tiratū says these outcomes are not inevitable. They are the result of longstanding inequities in housing, income, healthcare access and investment.
The Board is calling for sustained investment in kaupapa Māori and whānau-led solutions, accessible primary care, warm and healthy housing, and stronger accountability for Māori health outcomes.
Te Tiratū says Māori leadership and whānau voices must sit at the centre of any national response to child health, including decisions about funding, service design and prevention, as part of upholding Te Tiriti o Waitangi and mana motuhake in health.
[1] Source: Cure Kids, 2026 State of Child Health in Aotearoa New Zealand, March 2026 – national child health findings, including preventable hospitalisations, respiratory illness, rheumatic fever, mental health, deprivation, housing, and primary care access. Relevant pages: pp.4, 6-9
[2] Source: Te Tiratū IMPB, Monitoring Report to March 2025, 15 May 2025 – Waikato District asthma hospitalisation data: average of 215 Māori children aged 14 and under hospitalised for asthma each year between 2020-2023, 1.9 times the rate of non-Māori children. Relevant page: p.24. and Te Tiratū IMPB, Health Profile Volume 1: Key Indicators, 26 April 2024 – Waikato Māori deprivation, overcrowding, damp housing, mould, and primary care enrolment data and Te Tiratū, Community Health Plan – Refreshed Draft, 28 April 2026 – local town report themes around rural access, distance, transport, service availability, prevention, primary care connection and whānau voice.

What keeps Waikato rangatahi well & what gets in the way
In April rangatahi across our rohe shared their experiences of hauora using our dedicated Rangatahi Whānau Voice Survey. It offered an unfiltered snapshot of what wellbeing looks like in their everyday lives. This mahi is about something simple but powerful, listening.
Responses came from Kirikiriroa, Tokoroa, Te Awamutu, Te Kūiti, Ngāruawāhia, Taumarunui, and surrounding communities, each bringing their own realities of whānau life, identity, and access to health services.
What comes through strongly is that hauora for rangatahi is not defined by services alone. It is shaped in the spaces between home, school, sport, culture, and community. Many spoke about what keeps them well in simple, consistent terms like:
- playing sport
- kapa haka
- eating kai at home
- sleeping well
- spending time with friends
- being active in te ao Māori
- learning te reo
- attending marae-based Kaupapa
- being in the taiao
- or connecting through hunting, fishing, and diving
At the same time, rangatahi were clear about what sits beneath their wellbeing. Mental health featured consistently, alongside school pressures, relationships at home and with peers, and the ongoing stress of money, kai insecurity, and housing.
Safety, both at home and in the wider community, was raised alongside concerns about social media, gaming, vaping, and exposure to drugs and alcohol. For some, the ability to feel valued, understood, and culturally connected was just as important as more material needs. The picture that emerges is of a generation negotiating multiple layers of pressure while trying to stay grounded in identity and connection.
Access to health services was generally described positively, particularly where rangatahi had relationships with school nurses, practice nurses, GPs, counsellors, and other frontline providers. Many described services as friendly and welcoming, with comments reflecting a sense of ease when engaging with care. Telehealth was also mentioned as an option alongside in-person appointments, particularly for general practice and mental health support.
However, this accessibility is not experienced evenly. While some rangatahi reported being able to get appointments when needed, others pointed to gaps, delays, or limitations in what is available particularly in relation to mental health and youth-specific support.
In smaller towns especially, access feels more constrained, and transport was raised as a practical barrier to receiving care. Even where services exist, they are not always easy to reach or navigate.
When asked whether health services in their towns meet rangatahi needs, responses were mixed. Some felt services were working well enough, describing them as welcoming and supportive. Others were more cautious, noting that there is still room for improvement, or that services do not yet fully reflect what rangatahi actually need.
What is consistent across the kōrero is that rangatahi are clear that services need to reflect this reality not just in availability, but in how they are designed, delivered, and experienced.
These voices from rangatahi provide not only feedback on current services, but direction for future design. They point toward a system that is more relational, more culturally grounded, more accessible, and more responsive to the realities of young people’s lives in the Waikato.
They shared they value strong cultural foundations while trying to be resilient in the face of very real pressures and gaps in support. Rangatahi are already showing what wellbeing looks like in practice. The challenge now is whether systems will move to meet them there.
What whānau told us cannot be ignored
Last month our Whānau Voice surveys collected whakaaro from sixty-five whānau. What came back is not abstract data. It’s lived experience, spoken plainly and without filter.
The strongest thread running through their whakaaro is that hauora is never just one thing. Whānau are carrying multiple conditions at once, asthma alongside diabetes, mental health alongside work stress, chronic illness alongside caring for tamariki. It’s not isolated. It’s layered. And it’s constant.
One of the clearest messages is how hard it can be to actually get care when you need it. Even when whānau say “yes, I can access help,” the reality often sits underneath that answer. Wait times. Booking weeks in advance. Costs. Transport. Or simply deciding it’s too hard this time. Access exists, but it is stretched, delayed, and uneven.
Housing sits right in the middle of this. Whānau talked about cold, damp homes, poor ventilation, and babies living in conditions that worsen existing health issues. These aren’t separate from healthcare, they are part of it. For many, health starts in the home, not the clinic.
At the same time, whānau showed their inner wisdom of their own hauora. They know their conditions. They know what works for them. They know when to push through and when to adapt. This lived expertise is one of the most powerful things in our surveying. We’re witness to whānau managing complex situations with limited support, drawing on experience, whānau knowledge, and sometimes rongoā or lifestyle change to keep going.
There is also a clear imbalance in experience. Some whānau have steady, supportive relationships with services. Others are still navigating systems that feel slow, confusing, or unresponsive. The difference is not always need, it is often access, timing, and how well the system responds when it matters.
Mental health came through strongly, not as a standalone issue, but as a critical factor tied to everything else; pressure, money, work, whānau responsibility, and exhaustion. Whānau spoke about anxiety cycles, depression, and the effort it takes just to keep moving forward. Alongside that, they spoke about resilience and the way whānau, culture, and everyday practices hold people up when systems don’t.
What stands out most is the honesty. Our people did not soften their experiences. They spoke about long waits for surgery, the cost of going private, frustration with being unheard, and the emotional weight of repeating their stories. But they also spoke about what sustains them like kapa haka, whānau time, walking, gardening, marae, and being together.
These surveys are a reflection of how whānau are living right now, what is working, what is not, and what sits in between. Collected in a space of connection rather than formality, they carry a clarity that is hard to ignore.