
Keeping Māori health needs visible in funding decisions
Māori health leaders are calling for ethnicity to remain part of how primary healthcare funding decisions are made, warning that removing it risks overlooking the needs of Māori whānau.
Te Tiratū Iwi Māori Partnership Board and Te Taura Ora Iwi Māori Partnership Board represent more than 193,000 Māori across Waikato and Rotorua and are advocating for a funding system that reflects the realities of Māori communities.
The Boards say health funding is not just about numbers; it determines whether whānau can access the services, support and care they need.
“The way health capitation funding is designed matters. It must reflect the obligations of Te Tiriti o Waitangi and recognise the realities faced by Māori communities,” said Glen Tupuhi, co-Chair of Te Tiratū Iwi Māori Partnership Board.
“A funding model that does not recognise ethnicity risks making Māori health need invisible.”
The new primary care funding model considers factors such as age, deprivation, rurality and complexity of health conditions. However, ethnicity has been removed from the main funding formula, with an Equity Adjuster introduced as a temporary measure.
The Boards say equity funding should strengthen a fair system and not replace a formula that fails to recognise Māori health needs.
Research published in the New Zealand Medical Journal found ethnicity remains an important predictor of health outcomes, even after considering factors such as income, location and existing health conditions.
The study found Māori were 46% more likely than non-Māori to die from conditions that could have been prevented or treated through effective healthcare.
Te Tiratū and Te Taura Ora say Māori health inequities cannot be understood by looking only at poverty, location or illness.
“Ethnicity provides important information about health need and must remain part of how funding decisions are made,” said Hingatu Thompson, Chair of Te Taura Ora Iwi Māori Partnership Board.
The Boards are calling for assurance that Te Tiriti o Waitangi remains central to health funding decisions, that ethnicity continues to be recognised as a measure of health need, and that Māori health leaders and providers have a meaningful role in shaping future investment.
“If Māori health need is not visible in the funding model, it becomes easier for inequity to remain invisible across the health system,” Thompson said.
The Boards will write to the Minister of Health, the Hauora Māori Advisory Committee and Te Whatu Ora Health New Zealand to seek assurance that Māori health remains central to future funding decisions.
Te Tiratū and Te Taura Ora support greater investment in primary care, including stronger funding for GP services, rural communities, immunisation, prevention, early intervention and support for whānau managing long-term health conditions.

Waikato partnership puts whānau voices at the heart of health & social services
Image: Cabinet Minister Hon. Tama Potaka, Tumu Whakarae of Te Tiratū Iwi Māori Partnership Board Brandi Hudson and Jaye Wainui, Tumu Whakarae of Tamariki Tū Tamariki Ora
Te Tiratū Iwi Māori Partnership Board and Tamariki Tū Tamariki Ora have joined forces to strengthen the voices of whānau, achieve greater efficiencies while ensuring their lived experiences help shape future health and social services across the Waikato.
The collaboration will see Whānau Voice surveying by Te Tiratū integrated into the existing engagement Tamariki Tū Tamariki Ora and Rangitāmiro Whānau Ora Commissioning Agency has with whānau.
It will enable their feedback to be gathered naturally through everyday interactions with navigators and frontline kaimahi rather than through separate surveys to avoid fatigue.
Te Tiratū Tumu Whakarae Brandi Hudson said this move reflects a shared commitment to putting whānau at the centre of the service and remove silos.
“Our collaboration makes better sense. It’s about listening to whānau in ways that are respectful and meaningful. By working together, we can hear directly from whānau through the trusted relationships already in place and use those insights to advocate for better outcomes.”
Te Tiratū is working alongside Tamariki Tū Tamariki Ora to develop a streamlined approach that fits naturally within existing services and avoids placing additional demands on whānau. Hudson said she was impressed by the organisation’s integrated model of care after attending the recent launch of its new identity.
“You could see the pride and passion of the kaimahi in the room and their commitment to the whānau they serve. It’s a kaupapa with a thirty year whakapapa and deep roots with a clear vision for prevention and long-term wellbeing We’re looking forward to working together to ensure whānau voices are heard and acted on.”
Tamariki Tū Tamariki Ora supports more than 4,000 tamariki and whānau each year across Hamilton and the wider Waikato through an integrated network of housing, child protection, justice, disability, family violence and Whānau Ora services.
The partnership reflects a shared belief that better outcomes are achieved when services are informed by the voices and experiences of whānau themselves.
Chief Executive Jaye Wainui said the partnership reinforces the organisation’s commitment to designing services around whānau rather than organisational boundaries.
Together, the two organisations believe that by uniting, they demonstrate how Māori-led organisations can combine their strengths to create more connected, evidence-informed services that place whānau aspirations at the heart of decision-making.

More doctors closer to home for whānau in the Waikato
Image: University of Waikato’s New Zealand Graduate School of Medicine
Communities across Te Manawa Taki (Midlands) will play an important role in training future doctors of Aotearoa following official confirmation by the Health Minister of clinical placement locations for the proposed New Zealand Graduate School of Medicine at the University of Waikato.
The announcement includes successful iwi-led proposals in both the Tainui and Te Arawa waka regions, creating new opportunities to grow a local medical workforce and improve access to healthcare for whānau.
Across the Tainui waka rohe, North Waikato, Hauraki/Thames-Coromandel, South Waikato and Waipā/King Country have also been confirmed as Community Clinical Learning Centre locations, with Waikato Hospital serving as the anchor hospital for hospital-based placements.
The centres will provide medical students with opportunities to train in community, primary care and hospital settings, helping build stronger local workforce pathways and addressing doctor shortages in regional communities.
Waikato-Tainui Te Arataura Chair Tukoroirangi Morgan says the initiative represents a significant investment in local communities and the future health workforce. “The introduction of a third medical school is a game changer for our people,” he said.
In Te Arawa, a collective involving Te Taura Ora o Waiariki Iwi Māori Partnership Board has been selected to establish a Community Clinical Learning Centre.
For Māori communities, the initiative is about more than medical education. It creates pathways for whānau into medicine, strengthens Māori workforce development and helps ensure future healthcare services better reflect and understand the communities they serve.
As members of the Te Manawa Taki collective, Te Tiratū acknowledges the leadership of Waikato-Tainui, Raukawa, Hauraki, Maniapoto, Ngāti Hāua (Taumarunui) Te Taura Ora and their partners in securing opportunities that will benefit whānau across the wider region.
For Māori communities, this is about more than medical education. It is about creating pathways for our whānau into medicine, strengthening Māori and regional workforce pipelines, and ensuring communities have a greater voice in shaping the healthcare workforce of the future.
Under the proposed model, students will undertake training across community health services, primary care and hospital settings throughout the region. The programme is expected to welcome its first students in 2028, with community clinical placements beginning from 2029.

Whānau encouraged to send submissions to Pharmac before deadline
Pharmac is proposing to remove Māori and Pacific ethnicity equity criteria from access to important medicines used to treat type 2 diabetes, heart failure and chronic kidney disease. Read our media release for all the details.
These medicines help prevent serious complications including dialysis, amputations, heart attacks and early death. For many whānau, this is not an abstract policy issue it is about survival, quality of life, and equitable access to treatment.
Consultation closes at 5:00pm, Thursday 11 June 2026.
Te Tiratū is encouraging whānau, clinicians, providers and community leaders to make a submission opposing the removal of equity access pathways.
Use Our Free Submission Template
We have created a free submission template to make it easy for whānau to have their voices heard.
Simply:
- Download or copy the template
- Add your name and any personal comments
- Email it directly to Pharmac before 11 June 2026
Every submission matters.
Why This Matters
One of the largest Iwi Māori Partnership Boards in the country, Te Tiratū represents more than 121,300 Māori and is calling on Pharmac to immediately reconsider the proposal.
The ethnicity equity criteria were introduced in 2021 because Māori and Pacific peoples experience significantly higher rates of diabetes, cardiovascular disease and kidney disease, while also facing systemic barriers accessing medicines.
Te Tiratū Co-Chair Glen Tupuhi says:
“These medicines save lives and prevent devastating complications for whānau. Māori are diagnosed younger, become sicker earlier, and die sooner from preventable chronic illnesses. Equity pathways exist because the health system has not delivered equitable outcomes for Māori.”
Research and evidence presented through the Waitangi Tribunal Wai 2575 inquiry has already documented significant “prescription inequity” affecting Māori.
Te Tiratū is calling on Pharmac to:
- Retain ethnicity equity criteria for access to these medicines
- Release equity impact analysis publicly
- Demonstrate how Māori health outcomes will improve if criteria are removed
- Engage directly with Iwi Māori Partnership Boards and Māori health leaders
- Uphold Te Tiriti o Waitangi obligations in medicines policy decisions
Add Your Voice Today
Help protect equitable access to medicines for Māori whānau.
Use the free template, add your name, and email your submission to Pharmac before 5:00pm Thursday 11 June 2026.

Ngā Kōrero a te Poari: Maxine Ketu
Our Board Member Maxine Ketu (Ngāti Maniapoto, Waikato-Tainui), shares whakaaro on improving health outcomes for whānau and communities.
Why this kaupapa?
Firstly, why me?
I was appointed Pouārahi/General Manager of Ngāti Hāua Iwi Trust with a key focus on supporting our Trustees through the completion of our Treaty Settlement journey.
As that role evolved, I was appointed to the Waikato DHB Iwi Māori Council, and over the years I have continued alongside the evolution of Māori health representation to where we are today with Te Tiratū.
The responsibility I carry when representing Ngāti Hāua and our rohe is significant. For me, this mahi is about the difference between life and death for our people.
That understanding comes from lived experience. My own whānau experienced the impacts of rural isolation, poverty, limited access to healthcare, and the inequities Māori continue to face within the health system. Those realities contributed to the untimely loss of a loved one.
That was 11 years ago, but since 2014 I have walked beside many whānau who have experienced the same pain and loss. I have woven waka wairua for whanaunga taken too young, too soon. I have stood at nehu and helped lay our loved ones to rest when I know they should still be here.
My representation, my passion, and my commitment to this kaupapa all come from those lived experiences.
What does real change look like?
Real change starts with whānau feeling empowered to take charge of their own health and wellbeing. That looks like:
- having access to good health education and information
- understanding our own whānau and generational health histories
- feeling confident to ask questions and seek second opinions when needed
- not settling for poor treatment or mediocre care
- putting ourselves and our loved ones first
- making informed and healthy choices through ongoing learning
- knowing we have the right to demand high-quality care for ourselves and our whānau at all times
Real change also means the health system valuing the mātauranga, lived experiences and voices of whānau as part of healthcare assessment, treatment and follow-up.
We need a health workforce that is trained to recognise and address unconscious bias. This learning should not be optional, it should be embedded across all health education, professional training and ongoing development.
For our rural communities, real change means equitable access to healthcare no matter where you live. Communities that are far from hospitals and specialist services need secure, long-term investment that is protected across governments and political cycles. Rural whānau should not receive poorer outcomes simply because of where they live.
We also need stronger systems for accountability and learning. A national complaints and feedback system could help ensure concerns raised by whānau are heard, responded to, and used to improve services over time. The information gathered could help identify gaps in access, improve service delivery, strengthen professional practice, and ultimately lead to better health outcomes for our people.
What needs to stop, shift or grow?
We need to stop accepting inequitable outcomes for Māori and rural communities as normal.
The health system must be shifted toward one that truly listens to whānau, values Māori knowledge, and responds with compassion, accountability and equity.
We need to grow:
- investment in iwi-led health education and prevention
- culturally safe healthcare practices across the system
- unconscious bias training throughout health education and workforce development
- diversity within the health workforce, so our people can see themselves reflected in the system
- better access to healthcare services for rural communities
- stronger systems for listening and responding to whānau feedback and complaints
When whānau feel seen, heard, respected and supported, health outcomes improve. That is the future we should all be working toward.

Māori mental health inequities in Waikato demand urgent system reform
Te Tiratū represents approximately 121,000 Māori across the Waikato rohe, with around half under the age of 25. In our submission to the Government’s Mental Health and Wellbeing Strategy filed today we said the national mental health policy must be built from the realities of rangatahi Māori and whānau Māori and not retrofitted to them.
In rural Waikato, distress is not abstract. It is shaped by access barriers, workforce shortages, housing and income pressure, and the compounding effects of isolation. Te Tiratū argues that unless these conditions are addressed directly, the mental health system will continue to respond too late, and too often in crisis.
Our core message to Government
Te Tiratū is calling for a strategy that shifts from crisis response to prevention, from generic service design to Māori-led solutions, and from urban-centric planning to rural equity.
Our submission’s most critical recommendations are:
- Increase rural funding and expand telehealth capacity.
- Build and retain a rural mental health workforce.
- Address socioeconomic drivers of distress.
- Resource Māori cultural perspectives and whānau involvement.
- Support youth-led and community-based programmes.
The evidence from Tainui Waka Rohe
Our submission draws on our locality evidence base, which shows persistent and significant inequities in mental health outcomes across our region.
- Between 2017 and 2022, 16.0% of Māori aged 15+ in Waikato District experienced high or very high psychological distress
- Rising to 19.7% for Māori women
- Māori were 1.7 times more likely than non-Māori to experience high or very high distress
The data also shows the depth of unmet need:
- 5% of Māori reported a depression diagnosis
- 1% reported an anxiety disorder
- Māori were 1.9 times more likely than non-Māori to be hospitalised for mental or substance use disorders (2020–2023)
- Including 4.6 times higher hospitalisation rates for schizophrenia
- Around 225 Māori aged 15 to 44 are hospitalised each year for intentional self-harm
What must change in the system
We believe the current system is still too weighted toward crisis care, with insufficient investment in early intervention, rural access, and culturally grounded support.
Our submission says that meaningful improvement will only occur when services are designed closer to communities, delivered earlier, and shaped by a te ao Māori worldview and leadership.
We know workforce retention in rural areas is a critical pressure point because without it, access gaps will persist regardless of funding increases.
Treaty obligations and system accountability
A key concern of our submission is the limited visibility of Te Tiriti o Waitangi within the draft strategy, particularly Article 3 obligations relating to equity.
Without explicit Te Tiriti grounding, the strategy risks failing to address the structural drivers of inequity in mental health outcomes for Māori.
How accountability, investment, and service design are structured determines whether equity is achieved or not.
National context reinforces urgency
National data from Te Hiringa Mahara – Mental Health and Wellbeing Commission confirms the same pattern seen in Waikato, with 22.5% of Māori adults experiencing high or very high psychological distress, and 22.9% of young people aged 15–24 affected.
This aligns strongly with our locality findings and reinforces that rangatahi Māori are carrying a disproportionate burden of distress across the country.
Strategy alignment, but not yet sufficient
Our submission responds to the Ministry of Health New Zealand Draft Mental Health and Wellbeing Strategy 2026–2036, which focuses on prevention, access, workforce, and quality of care.
We support these directions in principle but argues they will not succeed unless they are explicitly grounded in Te Tiriti, rural equity, and Māori-led service design. Without this, the strategy risks maintaining existing inequities under a restructured framework.
Mental health reform will not succeed in Tainui Waka rohe if it continues to treat Māori as an “equity consideration” rather than the foundation of system design. The evidence shows that inequities are persistent, and the solutions are known. What is required now is investment, accountability, and a shift in power toward Māori-led, whānau-centred, community-based approaches.
Important References to inform the strategy:
- Te Tiratū IMPB, Hauora Māori Priorities Summary Report, here, pp.36-41 – Waikato Māori psychological distress, depression, anxiety, suicide, mental health hospitalisations, substance/alcohol-related hospitalisations and intentional self-harm data.
- Te Tiratū IMPB, Monitoring Report to March 2025 here, 15 May 2025, pp.22 and 25-26 – Māori access to primary and specialist mental health and addiction services, ED mental health waits, and commentary that services must remain culturally safe and whānau-friendly.
- Te Tiratū IMPB, Position Statement – Rangatahi Māori Mental Health, here23 September 2025 – Te Tiratū public position on rangatahi Māori mental health in rural Waikato, including rising distress, suicide risk, addictions, takatāpui youth pressures, rural isolation, service gaps, and the call for kaupapa Māori, whānau-led solutions.
- Te Hiringa Mahara – Mental Health and Wellbeing Commission, NZ Health Survey 2024/25 mental health and substance use data summary, 25 February 2026 – national context: 22.5% of Māori adults and 22.9% of young adults aged 15-24 experienced high or very high psychological distress.
- Ministry of Health, Draft Mental Health and Wellbeing Strategy 2026-2036 consultation, 8 April 2026 – consultation context and the four priority areas: prevention and early intervention, improved access, supported workforce, and quality/effectiveness of care.
60,000 children hospitalised each year with preventable illness
Te Tiratū Iwi Māori Partnership Board is backing urgent calls for action following the release of the fifth State of Child Health in Aotearoa New Zealand Report, which highlights worsening child health outcomes and persistent inequities for tamariki Māori.
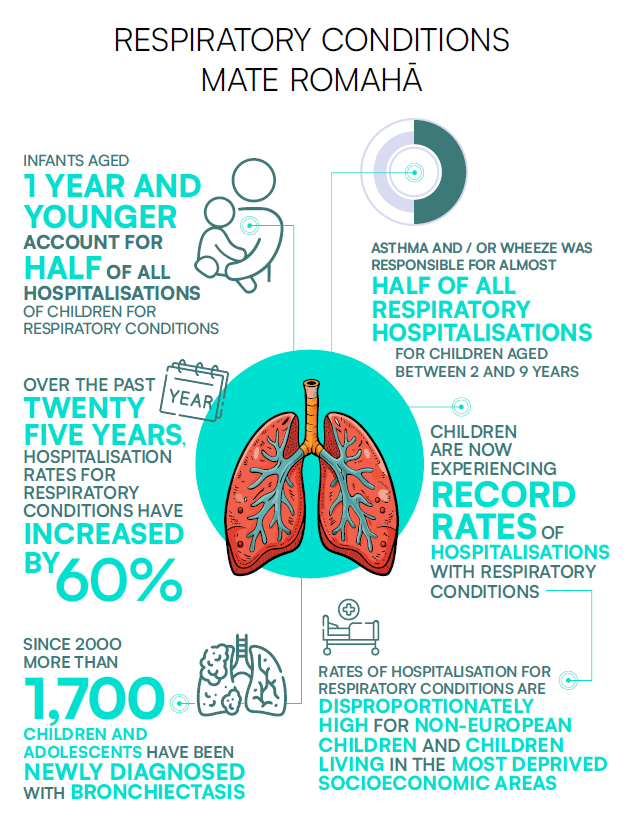
The report, produced by Cure Kids in partnership with the New Zealand Child and Youth Epidemiology Service at the University of Otago, shows around 60,000 children are admitted to hospital every year with illnesses considered preventable.
Respiratory hospitalisations have increased by 60 percent since 2000, with babies under one year old accounting for almost half of all admissions. Tamariki Māori continue to experience disproportionately high rates of respiratory illness and rheumatic fever.[1]
These national trends are already being felt across Tainui waka rohe. Local monitoring shows an average of 215 Māori children aged 14 and under were hospitalised for asthma each year in Waikato District between 2020 and 2023 1.9 times the rate of non-Māori children.
The figures reflect the wider realities many whānau are living with. Nearly half of Māori in Waikato DHB lived in the two most deprived deciles, almost one in four lived in overcrowded housing, 45 percent reported damp homes, 37.2 percent reported mould, and an estimated 17.5 percent of Māori were not enrolled with primary care.[2]
For rural whānau, the pressures are often even greater. Long travel distances, transport barriers, workforce shortages and delayed access to care can quickly turn manageable illness into hospital-level illness.
Te Tiratū says these outcomes are not inevitable. They are the result of longstanding inequities in housing, income, healthcare access and investment.
The Board is calling for sustained investment in kaupapa Māori and whānau-led solutions, accessible primary care, warm and healthy housing, and stronger accountability for Māori health outcomes.
Te Tiratū says Māori leadership and whānau voices must sit at the centre of any national response to child health, including decisions about funding, service design and prevention, as part of upholding Te Tiriti o Waitangi and mana motuhake in health.
[1] Source: Cure Kids, 2026 State of Child Health in Aotearoa New Zealand, March 2026 – national child health findings, including preventable hospitalisations, respiratory illness, rheumatic fever, mental health, deprivation, housing, and primary care access. Relevant pages: pp.4, 6-9
[2] Source: Te Tiratū IMPB, Monitoring Report to March 2025, 15 May 2025 – Waikato District asthma hospitalisation data: average of 215 Māori children aged 14 and under hospitalised for asthma each year between 2020-2023, 1.9 times the rate of non-Māori children. Relevant page: p.24. and Te Tiratū IMPB, Health Profile Volume 1: Key Indicators, 26 April 2024 – Waikato Māori deprivation, overcrowding, damp housing, mould, and primary care enrolment data and Te Tiratū, Community Health Plan – Refreshed Draft, 28 April 2026 – local town report themes around rural access, distance, transport, service availability, prevention, primary care connection and whānau voice.

What keeps Waikato rangatahi well & what gets in the way
In April rangatahi across our rohe shared their experiences of hauora using our dedicated Rangatahi Whānau Voice Survey. It offered an unfiltered snapshot of what wellbeing looks like in their everyday lives. This mahi is about something simple but powerful, listening.
Responses came from Kirikiriroa, Tokoroa, Te Awamutu, Te Kūiti, Ngāruawāhia, Taumarunui, and surrounding communities, each bringing their own realities of whānau life, identity, and access to health services.
What comes through strongly is that hauora for rangatahi is not defined by services alone. It is shaped in the spaces between home, school, sport, culture, and community. Many spoke about what keeps them well in simple, consistent terms like:
- playing sport
- kapa haka
- eating kai at home
- sleeping well
- spending time with friends
- being active in te ao Māori
- learning te reo
- attending marae-based Kaupapa
- being in the taiao
- or connecting through hunting, fishing, and diving
At the same time, rangatahi were clear about what sits beneath their wellbeing. Mental health featured consistently, alongside school pressures, relationships at home and with peers, and the ongoing stress of money, kai insecurity, and housing.
Safety, both at home and in the wider community, was raised alongside concerns about social media, gaming, vaping, and exposure to drugs and alcohol. For some, the ability to feel valued, understood, and culturally connected was just as important as more material needs. The picture that emerges is of a generation negotiating multiple layers of pressure while trying to stay grounded in identity and connection.
Access to health services was generally described positively, particularly where rangatahi had relationships with school nurses, practice nurses, GPs, counsellors, and other frontline providers. Many described services as friendly and welcoming, with comments reflecting a sense of ease when engaging with care. Telehealth was also mentioned as an option alongside in-person appointments, particularly for general practice and mental health support.
However, this accessibility is not experienced evenly. While some rangatahi reported being able to get appointments when needed, others pointed to gaps, delays, or limitations in what is available particularly in relation to mental health and youth-specific support.
In smaller towns especially, access feels more constrained, and transport was raised as a practical barrier to receiving care. Even where services exist, they are not always easy to reach or navigate.
When asked whether health services in their towns meet rangatahi needs, responses were mixed. Some felt services were working well enough, describing them as welcoming and supportive. Others were more cautious, noting that there is still room for improvement, or that services do not yet fully reflect what rangatahi actually need.
What is consistent across the kōrero is that rangatahi are clear that services need to reflect this reality not just in availability, but in how they are designed, delivered, and experienced.
These voices from rangatahi provide not only feedback on current services, but direction for future design. They point toward a system that is more relational, more culturally grounded, more accessible, and more responsive to the realities of young people’s lives in the Waikato.
They shared they value strong cultural foundations while trying to be resilient in the face of very real pressures and gaps in support. Rangatahi are already showing what wellbeing looks like in practice. The challenge now is whether systems will move to meet them there.
What whānau told us cannot be ignored
Last month our Whānau Voice surveys collected whakaaro from sixty-five whānau. What came back is not abstract data. It’s lived experience, spoken plainly and without filter.
The strongest thread running through their whakaaro is that hauora is never just one thing. Whānau are carrying multiple conditions at once, asthma alongside diabetes, mental health alongside work stress, chronic illness alongside caring for tamariki. It’s not isolated. It’s layered. And it’s constant.
One of the clearest messages is how hard it can be to actually get care when you need it. Even when whānau say “yes, I can access help,” the reality often sits underneath that answer. Wait times. Booking weeks in advance. Costs. Transport. Or simply deciding it’s too hard this time. Access exists, but it is stretched, delayed, and uneven.
Housing sits right in the middle of this. Whānau talked about cold, damp homes, poor ventilation, and babies living in conditions that worsen existing health issues. These aren’t separate from healthcare, they are part of it. For many, health starts in the home, not the clinic.
At the same time, whānau showed their inner wisdom of their own hauora. They know their conditions. They know what works for them. They know when to push through and when to adapt. This lived expertise is one of the most powerful things in our surveying. We’re witness to whānau managing complex situations with limited support, drawing on experience, whānau knowledge, and sometimes rongoā or lifestyle change to keep going.
There is also a clear imbalance in experience. Some whānau have steady, supportive relationships with services. Others are still navigating systems that feel slow, confusing, or unresponsive. The difference is not always need, it is often access, timing, and how well the system responds when it matters.
Mental health came through strongly, not as a standalone issue, but as a critical factor tied to everything else; pressure, money, work, whānau responsibility, and exhaustion. Whānau spoke about anxiety cycles, depression, and the effort it takes just to keep moving forward. Alongside that, they spoke about resilience and the way whānau, culture, and everyday practices hold people up when systems don’t.
What stands out most is the honesty. Our people did not soften their experiences. They spoke about long waits for surgery, the cost of going private, frustration with being unheard, and the emotional weight of repeating their stories. But they also spoke about what sustains them like kapa haka, whānau time, walking, gardening, marae, and being together.
These surveys are a reflection of how whānau are living right now, what is working, what is not, and what sits in between. Collected in a space of connection rather than formality, they carry a clarity that is hard to ignore.

Turning global learning into local action – World Indigenous Cancer Conference
Photo: Hinekura Ngataki, Principal Lead Health Sector and Clinical Engagement Kaitohutohu Clinical Advisor at Ngaa Pou Hauora oo Taamaki Makaurau Iwi Maaori Partnership Board with Dr Mataroria Lyndon, board member of Te Tiratū Iwi Māori Partnership Board.
Indigenous leaders, clinicians, researchers, community voices and Iwi Māori Partnership Boards, including Te Tiratū, have gathered in Tāmaki Makaurau for the 2026 World Indigenous Cancer Conference, hosted by Hei Āhuru Mōwai Māori Cancer Leadership Aotearoa.
It is the first time the global event has been held in Aotearoa. It brings a clear and urgent message, that the solutions to cancer inequities already exist and now it is time to act on them consistently to change our health system.
For Māori, the urgency is clear. We are more likely to be diagnosed with cancer and twice as likely to die from it. These inequities are long-standing and well understood. What is needed now is not more evidence of the problem, but commitment to implementing solutions.
One of our board members, Dr Mataroria Lyndon, attended the opening day. “The kaupapa goes beyond cancer. It is about equity, rangatiratanga and ensuring whānau are not left behind. The challenge is no longer identifying what needs to change but having the courage and accountability to make it happen.”
He believes we need to turn global learning into local action so that our next generation experiences a system that works for them, not against them.
Lived experiences shared at the conference reinforced how the system continues to fail whānau. Professor Jackie Kidd spoke about her Stage 4 bowel cancer diagnosis, highlighting how delayed screening and policy settings contributed to late detection. Sir Collin Tukuitonga also shared how difficult it was to navigate the system, despite decades of experience in health. Both stories pointed to the same issue: a system that is not designed around whānau needs.
A clear direction emerged. Stop researching barriers. Start implementing what works. That means placing mātauranga Māori at the centre of care, recognising rongoā Māori as part of prevention and wellbeing, and designing services that are whānau-centred and culturally grounded. It also means ensuring information is accessible and delivered in ways that connect with communities.
Practical examples showed what this can look like. Mobile screening services demonstrated how care can be brought closer to communities, removing access barriers. A dedicated rongoā Māori space reflected a more holistic approach to health that supports both prevention and healing.
International experience showed that change is possible. In Australia, Indigenous-led smoking programmes have significantly reduced smoking rates and helped tens of thousands of people quit. Across the Pacific, HPV vaccination programmes are showing early success.
However, many communities still face high tobacco use, limited screening access and increasing cancer rates, particularly where poverty and food environments are driving poor health outcomes.
Indigenous data sovereignty was also identified as critical, ensuring communities control how their data is used to shape better outcomes.
“Lasting change depends on genuine partnerships. These must be built on trust, shared decision-making and Indigenous leadership, not short-term or transactional approaches,” Dr Lyndon said.
“This conference comes at a critical time, as the Cancer Action Plan reaches its midpoint. Ongoing issues, such as screening age thresholds for Māori, highlight where equity has not yet been achieved and where action is needed.”