
Te Aka Whai Ora may be shut down but Māori health leaders are continuing its work

Te Aka Whai Ora may be gone, but the lessons remain. (Design: Tina Tiller).
Te Tiratū Iwi Māori Partnership Board member Dr Mataroria Lyndon reflects on the enduring importance of Māori leadership in hauora Māori following the disestablishment of Te Aka Whai Ora Māori Health Authority.
In his opinion piece for The Spinoff, Mataroria shares his reflections as a founding board member of Te Aka Whai Ora and considers the lessons from its short but significant journey.
He writes that while the organisation may have ended, the kaupapa of Māori decision-making, equity and whānau-centred health transformation continues through iwi Māori partnership boards, Whānau Ora commissioning agencies, Māori health providers and communities.
Mataroria says the future of hauora Māori must be built on enduring Māori leadership, strong partnerships and decisions made closer to whānau and communities.
Te Kūiti rural healthcare hub strained by rising demand

The Waikato Herald has featured the Te Kūiti Hauora Report by Te Tiratū Iwi Māori Partnership Board, highlighting the growing pressure on Te Kūiti’s health services as they support both the local community and surrounding rural areas. The article outlines the report’s findings on barriers to healthcare, including GP shortages, transport, affordability and workforce challenges, along with recommendations to strengthen primary care, maternity, dental and kaupapa Māori services. Health New Zealand said the report provides valuable insight that will help inform future planning for rural health services.
Keeping Māori health needs visible in funding decisions
Māori health leaders are calling for ethnicity to remain part of how primary healthcare funding decisions are made, warning that removing it risks overlooking the needs of Māori whānau.
Te Tiratū Iwi Māori Partnership Board and Te Taura Ora Iwi Māori Partnership Board represent more than 193,000 Māori across Waikato and Rotorua and are advocating for a funding system that reflects the realities of Māori communities.
The Boards say health funding is not just about numbers; it determines whether whānau can access the services, support and care they need.
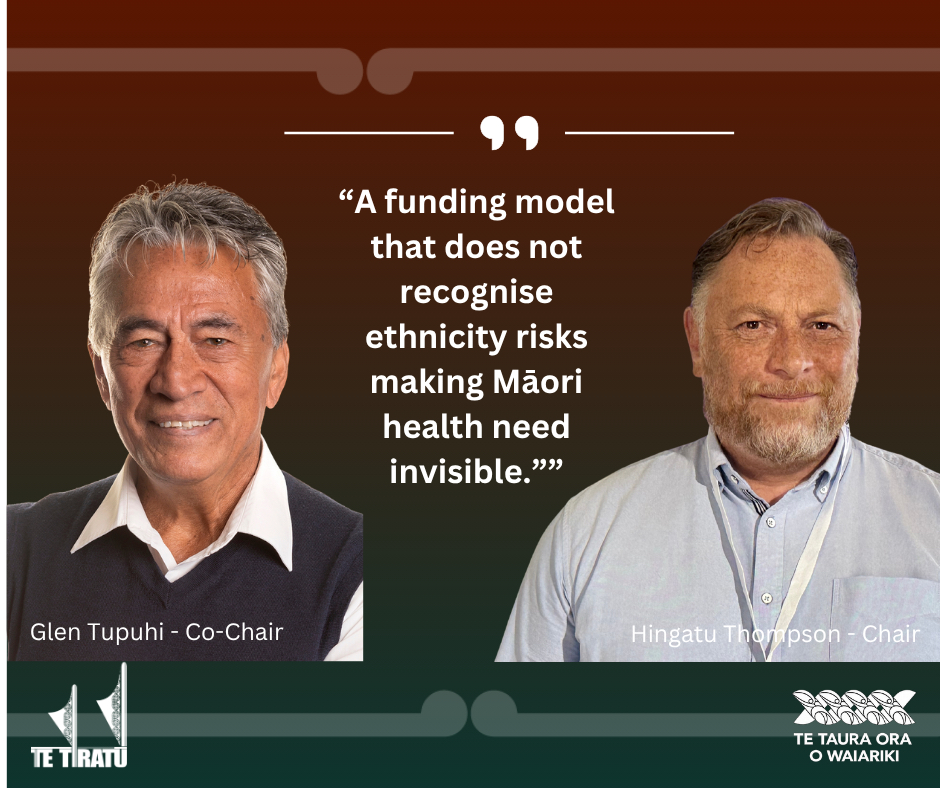
“The way health capitation funding is designed matters. It must reflect the obligations of Te Tiriti o Waitangi and recognise the realities faced by Māori communities,” said Glen Tupuhi, co-Chair of Te Tiratū Iwi Māori Partnership Board.
“A funding model that does not recognise ethnicity risks making Māori health need invisible.”
The new primary care funding model considers factors such as age, deprivation, rurality and complexity of health conditions. However, ethnicity has been removed from the main funding formula, with an Equity Adjuster introduced as a temporary measure.
The Boards say equity funding should strengthen a fair system and not replace a formula that fails to recognise Māori health needs.
Research published in the New Zealand Medical Journal found ethnicity remains an important predictor of health outcomes, even after considering factors such as income, location and existing health conditions.
The study found Māori were 46% more likely than non-Māori to die from conditions that could have been prevented or treated through effective healthcare.
Te Tiratū and Te Taura Ora say Māori health inequities cannot be understood by looking only at poverty, location or illness.
“Ethnicity provides important information about health need and must remain part of how funding decisions are made,” said Hingatu Thompson, Chair of Te Taura Ora Iwi Māori Partnership Board.
The Boards are calling for assurance that Te Tiriti o Waitangi remains central to health funding decisions, that ethnicity continues to be recognised as a measure of health need, and that Māori health leaders and providers have a meaningful role in shaping future investment.
“If Māori health need is not visible in the funding model, it becomes easier for inequity to remain invisible across the health system,” Thompson said.
The Boards will write to the Minister of Health, the Hauora Māori Advisory Committee and Te Whatu Ora Health New Zealand to seek assurance that Māori health remains central to future funding decisions.
Te Tiratū and Te Taura Ora support greater investment in primary care, including stronger funding for GP services, rural communities, immunisation, prevention, early intervention and support for whānau managing long-term health conditions.
Report raises alarm over strain on rural healthcare

Waatea has spoken with Te Nehenehenui Chief Executive and Te Tiratū Iwi Māori Partnership Board member Sam Mikaere about a new report revealing growing pressure on healthcare services in Te Kūiti.
The Te Kūiti Hauora Report, released by Te Tiratū Iwi Māori Partnership Board, highlights the challenges facing one of the central North Island’s key rural health hubs, including workforce shortages, limited GP access, transport barriers and rising healthcare costs.
The report describes Te Kūiti as a vital service centre supporting whānau across the wider Waitomo and Maniapoto rohe, with increasing demand placing pressure on local health providers and hospital services.
Sam Mikaere discusses why the report was commissioned and the need for stronger investment in rural health infrastructure, workforce development and Māori-led solutions to improve health outcomes.
The report calls for community-driven approaches that ensure whānau can access quality healthcare closer to home.
Te Kūiti carrying the weight of rural healthcare

King Country News has featured the first ever Te Kūiti Hauora Report by Te Tiratū Iwi Māori Partnership Board, highlighting the growing pressure on rural health services across the wider district.
The 48-page report examines the health needs of Te Kūiti and surrounding communities, finding that local providers are carrying increasing demand for GP services, maternity care, dental services and chronic disease management while supporting a predominantly rural population.
Drawing on community voices and local health data, the report identifies barriers including workforce shortages, transport, cost, childcare and limited appointment availability, all of which can delay access to healthcare. It calls for sustained investment in primary care, stable maternity services, expanded dental care, more specialist outreach clinics, improved rural transport and stronger kaupapa Māori services and whānau navigation.
Te Tiratū IMPB says practical, locally led investment is essential to ensure whānau can access timely care closer to home and reduce avoidable hospital admissions. The report also recommends that Ngāti Maniapoto be recognised as a partner in the design and delivery of health services to achieve better health outcomes for whānau across the King Country.

Waikato partnership puts whānau voices at the heart of health & social services
Image: Cabinet Minister Hon. Tama Potaka, Tumu Whakarae of Te Tiratū Iwi Māori Partnership Board Brandi Hudson and Jaye Wainui, Tumu Whakarae of Tamariki Tū Tamariki Ora
Te Tiratū Iwi Māori Partnership Board and Tamariki Tū Tamariki Ora have joined forces to strengthen the voices of whānau, achieve greater efficiencies while ensuring their lived experiences help shape future health and social services across the Waikato.
The collaboration will see Whānau Voice surveying by Te Tiratū integrated into the existing engagement Tamariki Tū Tamariki Ora and Rangitāmiro Whānau Ora Commissioning Agency has with whānau.
It will enable their feedback to be gathered naturally through everyday interactions with navigators and frontline kaimahi rather than through separate surveys to avoid fatigue.
Te Tiratū Tumu Whakarae Brandi Hudson said this move reflects a shared commitment to putting whānau at the centre of the service and remove silos.
“Our collaboration makes better sense. It’s about listening to whānau in ways that are respectful and meaningful. By working together, we can hear directly from whānau through the trusted relationships already in place and use those insights to advocate for better outcomes.”
Te Tiratū is working alongside Tamariki Tū Tamariki Ora to develop a streamlined approach that fits naturally within existing services and avoids placing additional demands on whānau. Hudson said she was impressed by the organisation’s integrated model of care after attending the recent launch of its new identity.
“You could see the pride and passion of the kaimahi in the room and their commitment to the whānau they serve. It’s a kaupapa with a thirty year whakapapa and deep roots with a clear vision for prevention and long-term wellbeing We’re looking forward to working together to ensure whānau voices are heard and acted on.”
Tamariki Tū Tamariki Ora supports more than 4,000 tamariki and whānau each year across Hamilton and the wider Waikato through an integrated network of housing, child protection, justice, disability, family violence and Whānau Ora services.
The partnership reflects a shared belief that better outcomes are achieved when services are informed by the voices and experiences of whānau themselves.
Chief Executive Jaye Wainui said the partnership reinforces the organisation’s commitment to designing services around whānau rather than organisational boundaries.
Together, the two organisations believe that by uniting, they demonstrate how Māori-led organisations can combine their strengths to create more connected, evidence-informed services that place whānau aspirations at the heart of decision-making.
Waikato Hospital ED death prompts iwi call for urgent action

In an interview with the NZ Herald, Te Tiratū Iwi Māori Partnership Board has called for urgent, system-wide action following the death of a patient at Waikato Hospital’s emergency department after a reported nine-hour wait.
The patient was found unresponsive in a waiting room toilet and could not be revived.
Te Tiratū says the incident reflects escalating, hospital-wide pressures rather than an isolated failure, including “access block,” staff shortages, and lack of inpatient beds causing flow breakdown across the system.
Board member Dr Mataroria Lyndon said the tragedy has deeply affected whānau, witnesses, and staff, and highlighted moral injury among clinicians working under sustained pressure.
Co-chair Glen Tupuhi said the review must go beyond the single incident to address wider system failures, including ED congestion, ambulance delays, and hospital capacity issues.
Health New Zealand has launched both an immediate clinical review and a full Serious Adverse Event Review.
A death in the ED waiting room is a system failure, not one bad day
A person died in a toilet in the waiting room of Waikato Hospital’s emergency department this week, after reportedly waiting nine hours to be seen. Staff performed CPR in front of a packed waiting room, full of whānau and tamariki. The patient could not be revived.
Three factors typically drive it. Patients wait too long for assessment and a definitive management decision by a senior clinician. Those who require admission remain in the emergency department because no inpatient beds are available. Delays in diagnostics, such as CT scans, slow diagnosis and treatment, create further bottlenecks throughout the hospital.
The consequences ripple well beyond the waiting room. Ambulances queue outside because they cannot hand patients over. Emergency clinicians cannot move patients into treatment spaces. Hospital wards remain full because people who are medically ready cannot be discharged while community and aged-care services are stretched. Pressure builds across every part of the system, from primary care through to hospital discharge. Simply adding more emergency department staff cannot solve a problem when there is nowhere for patients to go.
For whānau Māori, these system pressures compound barriers that already exist. Waikato Hospital serves a vast region extending far beyond Hamilton, where rural communities often face longer travel times, fewer primary care services and more limited access to urgent healthcare. Combined with the wider determinants of health, including poor housing and socioeconomic disadvantage, many whānau become seriously unwell before they even reach the hospital.
Understanding these realities does not excuse what happened this week. It helps explain why the burden of an overstretched system falls disproportionately on those who already experience the greatest inequities.
Two reviews are now under way: a rapid review and a serious adverse event review. Those processes must establish exactly what happened clinically, and that work should proceed without prejudice.
But our responsibility cannot end when those reports are released.
Te Tiratū will continue to scrutinise emergency department performance and the wider health system that sits behind it. We will continue advocating for meaningful implementation of the recommendations that emerge, for Waikato Hospital and for a health system under strain across the country.
The evidence for the solutions already exists, even if implementing them requires sustained investment and political commitment.
We need stronger primary and community healthcare, including Māori health providers delivering care closer to where whānau live. We need workforce planning that ensures graduates from the new Waikato medical school progress into specialist training and remain in our region. We need hospital infrastructure that provides safe clinical spaces rather than relying on corridors and waiting rooms. We also need better information sharing across primary care, community providers and hospitals so patients are not forced to repeat their story every time they encounter another part of the system.
To whānau who may now feel anxious about seeking care, please do not let this tragedy stop you from accessing health services when you need them. Delaying care carries risks of its own. If your condition is not an emergency, your GP, community pharmacy, telehealth services and Māori health providers remain important options. If it is an emergency, please still come to hospital.
As winter deepens, we can all help reduce pressure on the health system by getting influenza and Covid-19 vaccinations, keeping childhood immunisations up to date to protect against serious vaccine-preventable illnesses such as whooping cough and pneumococcal disease, staying home when unwell, and checking in on kaumātua and those living with chronic health conditions.
A whānau has lost someone they loved. We owe them, and the staff who tried to save them, more than sympathy. We owe them a health system that learns from this tragedy and is better because of it.
Dr Mataroria Lyndon (Ngāti Hine, Ngāti Wai, Ngāti Whātua, Waikato) is a member of the Te Tiratū Iwi Māori Partnership Board, director of population health and equity at Tend Health, and senior lecturer at the University of Auckland’s Centre for Medical and Health Sciences Education.
Māori health leaders respond after person dies waiting in Waikato Hospital

A Whakaata Māori News report has highlighted renewed concern about pressure on Waikato Hospital’s emergency department following the death of a patient after a reported nine-hour wait for care.
Lady Tūreiti Moxon, managing director of Te Kohao Health, said the impact of the tragedy would extend well beyond the hospital, affecting the patient’s whānau, hospital staff, and others who were present. She said long emergency department delays have become distressingly common.
Te Tiratū Iwi Māori Partnership Board, also expressed condolences and emphasised that no whānau should endure the trauma of losing a loved one while waiting for emergency care.
Board member and Hauraki PHO chair Glen Tupuhi said the focus must be on understanding systemic failure and preventing recurrence, noting that Māori experience disproportionate harm within the health system, including for rurally based whānau who face added barriers such as travel and long wait times.
Rangatira call for urgent systemic reform after autistic child case exposes serious agency failures
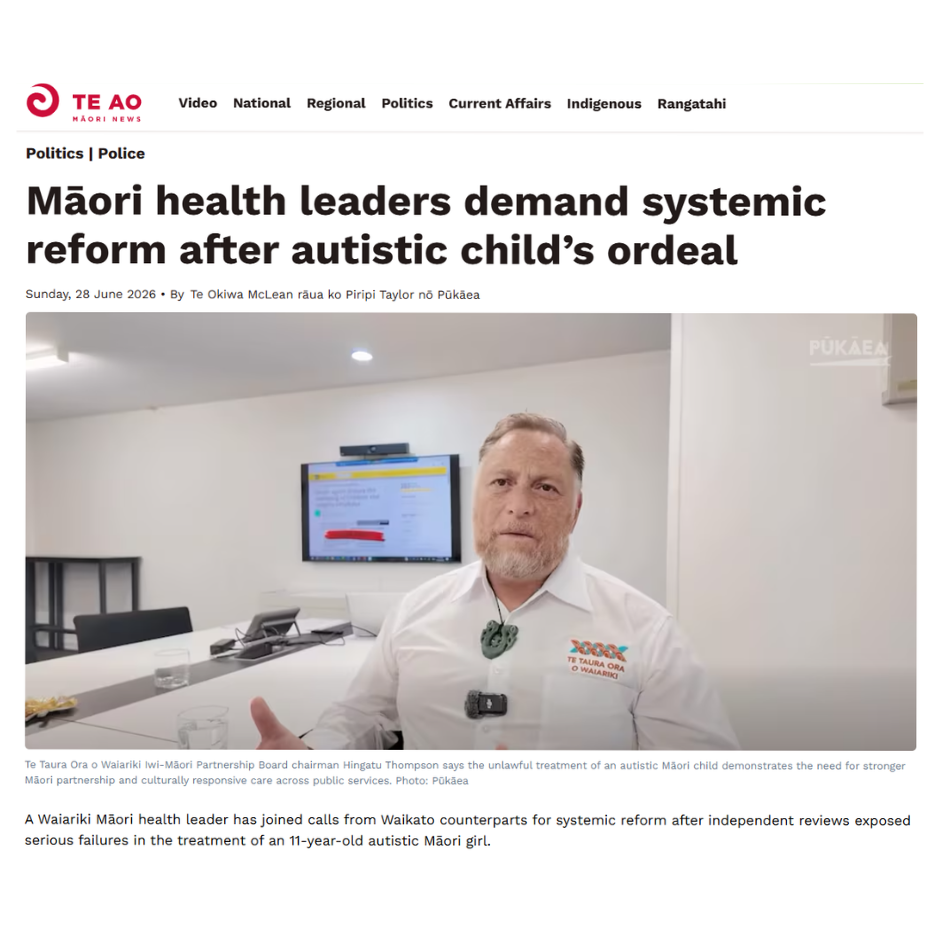
Māori health leaders including Te Taura Ora o Waiariki Iwi-Māori Partnership Board, Te Tiratū Iwi Māori Partnership Board and Lady Tūreiti Moxon are calling for urgent systemic reform following two independent reviews into the treatment of an 11-year-old autistic Māori child. Whakaata Māori reports the findings revealed multiple agency failures, including misidentification, unlawful restraint and inappropriate medication, prompting renewed demands for accountability, a formal Government apology, stronger Māori partnership in frontline services and disability system reform.