
A death in the ED waiting room is a system failure, not one bad day
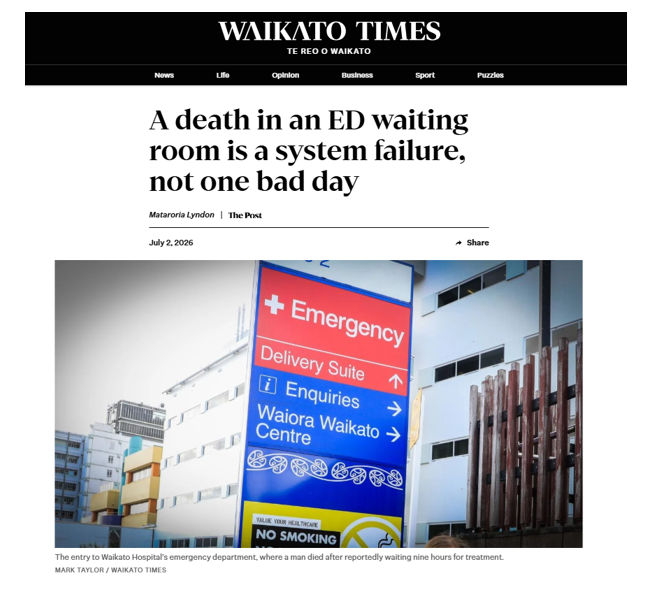
A person died in a toilet in the waiting room of Waikato Hospital’s emergency department this week, after reportedly waiting nine hours to be seen. Staff performed CPR in front of a packed waiting room, full of whānau and tamariki. The patient could not be revived.
Three factors typically drive it. Patients wait too long for assessment and a definitive management decision by a senior clinician. Those who require admission remain in the emergency department because no inpatient beds are available. Delays in diagnostics, such as CT scans, slow diagnosis and treatment, create further bottlenecks throughout the hospital.
The consequences ripple well beyond the waiting room. Ambulances queue outside because they cannot hand patients over. Emergency clinicians cannot move patients into treatment spaces. Hospital wards remain full because people who are medically ready cannot be discharged while community and aged-care services are stretched. Pressure builds across every part of the system, from primary care through to hospital discharge. Simply adding more emergency department staff cannot solve a problem when there is nowhere for patients to go.
For whānau Māori, these system pressures compound barriers that already exist. Waikato Hospital serves a vast region extending far beyond Hamilton, where rural communities often face longer travel times, fewer primary care services and more limited access to urgent healthcare. Combined with the wider determinants of health, including poor housing and socioeconomic disadvantage, many whānau become seriously unwell before they even reach the hospital.
Understanding these realities does not excuse what happened this week. It helps explain why the burden of an overstretched system falls disproportionately on those who already experience the greatest inequities.
Two reviews are now under way: a rapid review and a serious adverse event review. Those processes must establish exactly what happened clinically, and that work should proceed without prejudice.
But our responsibility cannot end when those reports are released.
Te Tiratū will continue to scrutinise emergency department performance and the wider health system that sits behind it. We will continue advocating for meaningful implementation of the recommendations that emerge, for Waikato Hospital and for a health system under strain across the country.
The evidence for the solutions already exists, even if implementing them requires sustained investment and political commitment.
We need stronger primary and community healthcare, including Māori health providers delivering care closer to where whānau live. We need workforce planning that ensures graduates from the new Waikato medical school progress into specialist training and remain in our region. We need hospital infrastructure that provides safe clinical spaces rather than relying on corridors and waiting rooms. We also need better information sharing across primary care, community providers and hospitals so patients are not forced to repeat their story every time they encounter another part of the system.
To whānau who may now feel anxious about seeking care, please do not let this tragedy stop you from accessing health services when you need them. Delaying care carries risks of its own. If your condition is not an emergency, your GP, community pharmacy, telehealth services and Māori health providers remain important options. If it is an emergency, please still come to hospital.
As winter deepens, we can all help reduce pressure on the health system by getting influenza and Covid-19 vaccinations, keeping childhood immunisations up to date to protect against serious vaccine-preventable illnesses such as whooping cough and pneumococcal disease, staying home when unwell, and checking in on kaumātua and those living with chronic health conditions.
A whānau has lost someone they loved. We owe them, and the staff who tried to save them, more than sympathy. We owe them a health system that learns from this tragedy and is better because of it.
Dr Mataroria Lyndon (Ngāti Hine, Ngāti Wai, Ngāti Whātua, Waikato) is a member of the Te Tiratū Iwi Māori Partnership Board, director of population health and equity at Tend Health, and senior lecturer at the University of Auckland’s Centre for Medical and Health Sciences Education.
Waikato Times cover childhood immunisation rate rise as Māori-led health approaches deliver results

The Waikato Times has highlighted Waikato’s significant improvement in childhood immunisation rates, with Te Kōhao Health and Te Tiratū Iwi Māori Partnership Board recognising the impact of trusted Māori providers, whānau-centred outreach and community-based vaccination services. Board member Dr Mataroria Lyndon said the progress was encouraging but stressed continued investment is needed to close the remaining equity gap for Māori tamariki and achieve the Government’s 95% immunisation target.
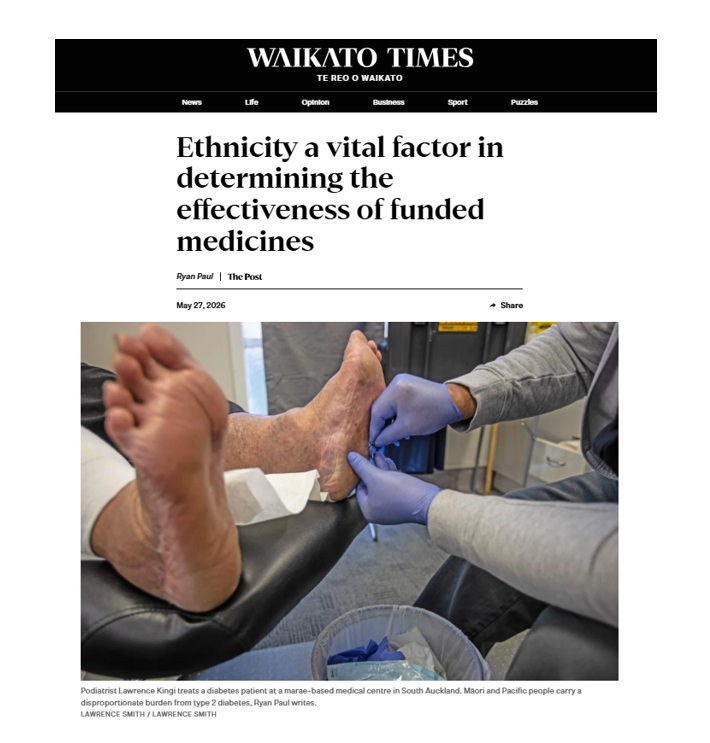
Ethnicity a vital factor in determining the effectiveness of funded medicines
Associate Professor Dr Ryan Paul, a clinician and technical expert advisor to Te Tiratū, explains why ethnicity should be a criterion for access to funded medications in Aotearoa New Zealand. [This think piece also appeared in The Post and The Press]
He says it is important to look at the evidence objectively. Māori and Pacific peoples are at least 2–3 times more likely to develop type 2 diabetes, acquire complications, and die prematurely from those complications than other New Zealanders.
“Pharmac’s volte-face to then remove the ethnicity criterion suggests that it was either ineffective or unfair, yet no public impact assessment or scientific explanation has been provided,” Dr Ryan Paul says.
Te Tiratū is encouraging whānau, clinicians, providers and community leaders to make a submission opposing the removal of equity access pathways.
Use Our Free Submission Template
We have created a free submission template to make it easy for whānau to have their voices heard.
Simply:
- Download or copy the template HERE
- Add your name and any personal comments
- Email it directly to Pharmac before 11 June 2026
The consultation closes on 11 June 2026.